The UK government is drawing up guidance for schools regarding trans kids and some of what they’re putting together has been leaked. You might think this has nothing to do with CRPS or any other of my multi-systemic chronic conditions that I write about here, but research has found all sorts of links, so it’s complicated and would warrant a whole other post, …but it’s also harder to be heard by doctors if we’re women, if our skin is any colour other than ‘white’, if English isn’t our first language, …if we’re trans… When othering is written into legislation it reinforces stereotypes of Other, Different, Not ‘Normal’. When that is part of our culture it is below our radar, internalised, part of our ‘normal’ world view. It impacts our perceptions of people with certain attributes in a way that doesn’t feel like we’re othering.
As a disabled person I’m acutely aware that the view of a disabled person is someone in a wheelchair. If we stand up we’re stared at. If we walk to and from a disability bathroom we are frowned at. If we park in a disabled bay we risk getting shouted at. I’ve found that if I wear a pretty dress and make-up in my wheelchair and it becomes apparent that the able-bodied person I’m with is my partner.. I get gaped at.
Our brains have evolved to believe a thing the more we see or hear it. Way back it was incredibly useful with that whole survival thing. Nowadays it means that the more we read something in headlines the more we think it’s true, the more we hear comments about groups of people – the more our stereotype gets shaped, and no matter how intelligent or academic we are this is still a Thing. Frustratingly! This would mean that even highly educated academics working in this field are not immune. So yes, politicians are also not immune.
Knowing this we have to approach this stuff incredibly cautiously. It’s like learning to draw where the first thing you have to learn is how to look. We see objects, but looking to observe new things about the object we already think we know is a hugely different approach. You have to first accept that maybe what you ‘know’ about that glass bottle in the still life arrangement isn’t enough.
A few lines to describe a bottle in front of me but without really looking at it so that it’s more from our stereotypical assumptions and with uninformed perspective errors.
One of the hardest things an art teacher has to do is get their students to realise that a lot of their drawing is from their head – from what they ‘know’ about the object. The hurdle is convincing them to truly observe and be open to learning about the object that they genuinely believe they already know. In art, as in academia, we learn that we cannot assume that what we think we know is correct. It takes effort to do this but if we want accurate representation it’s worth it.
A quick pencil sketch of the same bottle from actually looking and observing the object. There is a little more accuracy, and more detail and context but still some ‘wonky’ness.
So there’s a difficulty recognising that what we ‘know’ might not be sufficient or indeed even accurate.
In addition to that, politicians are often not specialists in the UK, or at least not specialist in the area they’ve been assigned. As chronically ill peeps we know all too well how this can impact awareness and understanding – the difference between talking to our General Practitioner or a tertiary level specialist about our complex condition is so utterly different it’s like being in a whole different world – although our GPs have been trained in general health information, it just doesn’t cover our specialist conditions. Our politicians are writing legislation based on what they have absorbed about the topic generally from society and from others around them, unlike our GPs it’s not even from any general training. As any of us disabled peeps know, societal stereotypes can be wildly inaccurate and no amount of excellent research and information out there will help if they don’t seek it out to properly inform themselves.
The legislation is supposed to be helpful, from one angle of generalised cis-parents point of view; but it separates, Others and harms the kids it should be protecting. It tells them and teaches everyone around them that they are different, that not having the same rights as others is appropriate, that being themselves is inappropriate and needs to be managed by other people who are not like them, that privacy and well-being are not priorities in their case which marks them ultimately as ‘lesser’. Their peers will learn this alongside them and grow up to be doctors, bankers, councillors,… whose internalised opinion of different groups of people will begin to inform their decisions before they’ve even met the individuals and, don’t forget, without them even clocking it’s happening, let alone how impactful that is.
It takes hard work to pick apart which bits of our understanding is fact-based and which bits have been absorbed by our brain as a truth simply because we’ve heard it so many times. But when writing legislation that impacts a group that they are not a part of, it is imperative that they do the work.
They don’t have time to do the work. They know what’s best. Right? ?
When trans kids are not supported, many more of them turn to suicide to escape the trauma. This legislation in progress does far more damage than ‘just’ not support them. Legislation that will lead to child suicides is horrific. Death is unfixable.
If you are impacted or know someone who is, here are some links recommended by some people in the know:
Hello all, I’ve been rarely posting because of the shift in my health. I took a blog-break when I moved house but when I passed out on a concrete floor back in January 2017 my whole life changed. Aaaaaall my symptoms got worse and I got a few new ones thrown in for free. Skipping the details for now because it’s not what I want to talk about. I’m following on from my last post which wrote itself when I ran out of optimism.
Like the psych’ grad I am I saw my reaction to desperate times and the devastating loss of hope and knew I needed to step back and look at a bigger picture as small changes were not going to impact anywhere near enough. The scientist in me said ‘as there is no medical support… where else can I look for medical help?’
So I was looking into alternatives and I have followed through on that. I waited before saying anything because it’s an unknown and I wanted data. I now have some, albeit early stages, which I can share with you.
For health conditions encompassing the functionality of whole systems we are often let down by the reductionist approach of mainstream Western medicine. Don’t get me wrong, it’s awesome in so many ways, but when it comes to those of us with long-standing tangled and complicated systemic dysfunctions and interactions it simply doesn’t work for the chronic aspects of our ill-health.
When complex patients present to doctors we have an overwhelming array of symptoms that don’t appear to make any coherent sense. That prompts them to question our reliability at self-reporting and to wonder if there are non-physical reasons causing us to list so many things. Even if they do believe us they are trained to triage the list of issues, pull out the most concerning one and address that. But trying to address one symptom as if it is a standalone issue doesn’t make the picture any clearer. It’s like stepping in close to a painting and looking at the left eye, the fabric, that pudgy cherub – you have to step back and take in more pieces of the picture to see what it actually is.
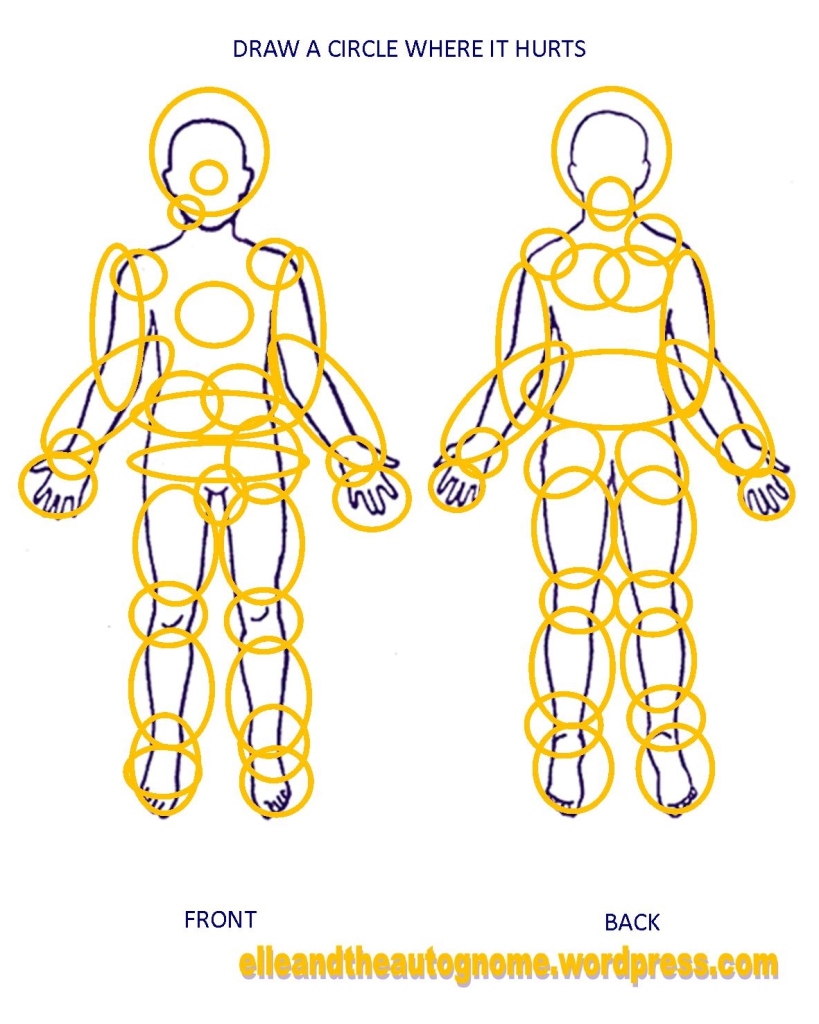
This pic was created regarding pain but our array of other symptoms is this messy too!
Description: A diagram of a human form, both front and back. At the top it says “draw a circle where it hurts”. There are many many circles drawn all over both!
Occasionally we might get referred to a specialist who might know more and be able to give us more insight. In my experience this sometimes is of no help if the referral area was a bad guess, but can involve a fabulously coherent conversation for once, a practitioner who not only listens and takes what we’re saying on board but also believes us and can explain some of why this is happening to us, then they write a letter to the GP who shrugs and files the letter. The end.
The symptoms and poor quality of life continue.
And the problem here is not just that there is no treatment, it’s not even that there often is no recognition of the issues that specialists have pointed out we’re dealing with or even belief in the diagnoses the specialists have made, it’s the fact that if left unaddressed our bodies are left working harder, continuously, with no medical assistance so our fuel gets depleted and we can’t replenish it quick enough to keep up. We are spiralling but we are shelved by our GPs as if our symptoms are stable.
Most obvious in my case has been the downward spiral of never-enough-neurochemicals. I wrote about my attempts to help this here. It helped noticeably by treating the symptom but it didn’t address the underlying cause and as it continued to spiral it was no longer enough to make a difference. It’s hard to treat an underlying cause when your GP has no interest in finding out what that cause is.
Description: A sketch. On one side of a desk a doctor is waving a hand around saying “We are here to treat symptoms and side effects. That is all. I do not want you researching for causes”. On the other side of the desk the patient is doing a head-desk.
I’m specifically trained in research. I’m good at this shit. I’m a scientist so I read information and take it as just that. I never do the thing GPs are afraid of patients doing when we look for information – I don’t think that I have the thing I’ve just found information on. What I do think is that I’ve just found some information that teaches me more about the biological mechanisms that are dysfunctioning in my body but I never think ‘and therefore this is me’. For that I need a medical practitioner who can suss the reason that my body is doing similar things. It can be dangerous to assume, which is why doctors tend to whinny and rear when a patient says they’ve been looking online but, in my best Bill and Ted voice: ‘it’s most tiresome’!
It’s tiresome because many expert patients are actually trying to share useful data and information with a doctor who is fundamentally opposed to taking anything the patient is saying seriously.
So, yeah. I needed someone who would take a functional approach and look at my symptoms from a systems wide perspective. I was aware of functional medicine in the US but didn’t know much about it. Was it going to be the perspective I was looking for? Were they medically trained at all or just functionally trained random peeps?
I learnt that a functional doctor is indeed a doctor, a functional nutritionist is a trained nutritionist, a functional neurologist…you get the idea. They’re Proper! Aaaaand they take the systemic approach, yeeeeeaaaaaaah!
At this point I got stuck into looking online…
It’s made its way over to Europe and more. Practitioners have their own array of specialisms which, happily, include things like autoimmune disease, chronic pain, chronic disease… This was looking more and more hopeful.
I found so many practitioners in my locality that I got to choose who I saw by the areas they had trained in to increase the chance that they would understand complex aspects of my condition.
I emailed a functional nutritionist (i.e. fully qualified nutritionist who has then additionally trained in the functional approach and specialist areas) who is just ten minutes down the road from me. As I was going to be paying for the appointment I wanted to check they were a good match beforehand so I included bullet points about me, my health and the gaping holes in my current healthcare that I needed to fill. I ended with “…if you feel that this is not a good fit for you I’d really appreciate any recommendations you have for someone you feel would be a great fit for this kind of scenario and complexity.” because who wants to pay for someone who isn’t appropriate.
We scheduled a phone call to cover what I was looking for, my health issues, what she has to offer me etc. – no cost to me
She sent me some questionnaires online, simple tick-box ones, based on the themes apparent to her from our phone conversation. – also no cost to me
I sent her my medical history as I already have it in a neat little (hah! okay, huge) table in a saved document. She’s used to this as so many complex patients have already created tables in the hope that the information will help doctors to hear what they’re saying <sigh> .
We scheduled a 1.5 hour assessment. She came to my home last November (we had the windows open for a through breeze and wore masks as I have to shield from COVID). She stayed an extra half hour because my health situation is so complex. Thank goodness she is totally used to complex health issues because it’s people like me who tend to go to see functional practitioners. The sad bit is that the reason we go to see them is because we fall through the nets of conventional medicine.
My experience of that assessment was akin to talking with a fellow patient. As she’s trained from a systemic perspective all the things I was saying made sense to her. She was unsurprised, she wasn’t confused by the diverse array of symptoms, she didn’t question the reality of what I was describing, she didn’t distrust me or think I was hysterical. She didn’t hear how knowledgeable I am and then automatically assume I’ve been self-diagnosing online. Like a fellow patient she heard everything I said, believed it, knew it to be true, cared about it, then on top of that I found that I could use all the technical medical jargon instead of explaining stuff because she knew it already from her relevant areas of training! I found I could just skip past that big chunk of any appointment with a new practitioner because I didn’t have to explain anything! We could just cut to the main issues and get on with it. My partner was there with me to help when my brain slipped away but because I could skip all the taxing explaining and just talk about what is effectively my specialist subject these days, I made it through the appointment without neuro downsliding and could keel over and recuperate afterwards. In fact he said to me afterwards that he didn’t understand most of what we were saying to each other.
What came out of that assessment was a report on my health situation from a functional and systemic perspective with recommendations for any exercises, tests, supplements etc moving forward.
Key things to note with this is that they are only recommendations – whether I follow through with any of them is entirely up to me. This is a good thing as a lot of the tests still get sent to the US so they are expensive. The report was sent to me so I can choose whether to share it with my GP or not.
The key priority for me that came out of this was that I have chronic brain inflammation. Very clearly so. Systemic inflammation is a part of CRPS, I’ve known this for a long time, but there appear to be different subtypes of CRPS (still not yet pinned down) and I am one of those patients who rarely has any visible symptoms of my primary pain condition. There are many other patients who continue to experience swelling beyond the acute stage as a significant part of their chronic pain response. The only visible signs I occasionally get are red spots on my knees warning me that I’ve done too much (and I’m too darn practiced at pacing to do that unless it’s a big occasion) or the burning red of my periodically on-fire toes. So, I figured, inflammation can’t be that bad in my body, right?
Oops.
Back in 2008 I stopped studying because my brain wasn’t playing ball any more. When I pushed myself to complete my research before the qualification timed out I regularly lost my brain. Doctors had no interest in me earnestly informing them that if I use my brain I lose it. Even when I lost three months to it and could not process words or think straight all that time. I guess it’s testimony to my skills and knowledge that I got my Masters degree under those conditions. Yikes! And now, 13 years later I find out the never-ending downslide of my brain functionality that I’ve been asking for help with has been inflammation….that has never even been considered let alone addressed?!
The other clear issue was regarding my neuro-mediated immune responses to ‘normal’ environmental things. Western medicine had also found this and prescribed a repeat prescription anti-histamine. Effectively saying my brain is an eejut and here’s how to calm the stuff it tells my immune system to do. Functional medicine takes a step back and considers all the information to look for clues as to why my body is doing this. Increased intestinal permeability is a likely issue so then we look at what we could do that might help reduce permeability somewhat.
Description: very rough sketch of my face. My eyes are crossed. There are three question marks around my head.
And this is why I need functional healthcare. Desperately.
The functional nutritionist gave me some diet variations to test out which helped a bit, but initially barely a drop in the ocean. The specific brain supplements however, wow! Significant improvement. Even though it’s still a very small improvement overall, it has nonetheless made a significant impact on my quality of life. Let’s face it, we’re talking many years of chronic brain inflammation and that has no easy fix. The supplements are expensive and there is no pressure to try any of the suggestions she’s made but I’m so glad I did. Once I got to the low histamine diet I realised that not only did that also help but that when reading up on the issue that it basically lists, in weirdly precise detail, all my weird and mysterious symptoms that had previously made no sense to me. Okay then. More knowledge is helpful.
Next stage: more tests. I’ve left this til now because it’s expensive. After the tests arrived we were ready to schedule but the main blood array is going to tell us more if they can see the impacts… so I’ve got to return to the impactful stuff. Boo and hiss! If I’d been up for the expense earlier I could have got them out of the way and then found the things that improve my functionality. As it is I’m gonna have to knowingly lose functionality for a while and that’s not gonna be fun. At least it will be a temporary situation but ugh!
A poem just wrote itself. Fell from my head to the page, line by line. It shows why I am currently looking at alternative medical thoroughfares. More on that anon. Meanwhile, here is what my brain just spewed. I’m off to put the kettle on so I can recuperate in my inbuilt Brit way whilst looking out at the back garden. xx
Dark Light
There is no light, no hope
No help. No Way.
My body doesn’t function properly
It’s invented it’s own erroneous ways of being.
It makes the wrong calls. Over and over.
Adds new nonsense to the way it reacts
To activity, both physically and cognitively.
My dysfunctional neurology is the commander of a team of systems that follow its every word
Pain is incessant. Screaming, slicing, throbbing. Relentless
An array of functional oddities barrage me all day
Every day.
Every night.
Every every.
Immune system freaks out at the existence of mundane things
Nervous system spins and twists, making me drop, making my brain and body shut down
In July many pandemic restrictions were lifted here in England (Northern Ireland, Scotland and Wales are still keeping various protections in place for now1). People are mixing more and they are doing so without taking as many (or in some cases any) precautions to protect others from the virus because 65%2,3 of the entire UK population have received 2 doses of SARS-CoV-2 vaccines. Much of the general population feel that all that can be done has been done and beyond that they weigh up being stuck with protection measures against living more ‘normal’ lives again and decide that they are prepared to take that risk and hope for the best. This is their choice for their bodies. The problematic part is when we vulnerable patients are expected to be at the same amount of risk and therefore to make the same choice. Vulnerable patients are at much greater risk. So although our friends and families are expecting to be able to see us again we’re having to shield even more than before because when the general population started mixing more our chance of being exposed to the virus increased dramatically. Yet often when we say we still can’t mix without lots of precautions it’s met with surprise or confusion. It’s hard for us to explain the complexities of our conditions and why we’re so different from the general population. I hope to help a little with that…
Asa case example, here is why I can’t risk catching SARS-CoV-2…. 1. My immune system is compromised so the vaccine doesn’t protect me as much. It will offer me some protection against hospitalisation and death but not as much as it would if my immune system was fully functional. (The UK government website generalises so this patient subgroup is not mentioned regarding the different risk4, but it is established that a natural deterioration of immune system effectiveness (immunosenesence) occurs with age and that the more the system is compromised the less effective vaccines are as a result5,6,7,8. Those with a compromised immune system experience this whatever age they are with the added complications of system dysfunctions and multiple condition impacts). 2. As my immune system is compromised – a lower viral load (smaller amount of virus) presents just as much risk to me as a high load. So situations that are generally seen as ‘less risky’ to others are still high risk to me. 3. My immune system is dysfunctional because a part of my brain is dysfunctional. My neurological condition is the reason why my immune responses are so, um, well, ridiculous quite frankly. 4. I have chronic systemic and brain inflammation. Covid can cause an inflammatory cytokine ‘storm’21 which, when added to pre-existing inflammation, can prove to be fatal. This is another factor that increases my risk of death from Covid. 5. My nervous system is a quick-learning so-and-so. If a new physiological behaviour shows up, my nervous system learns it within 1-2 weeks. The learned new default is the new way of working. It does not go away. My body learns it and goes “this it how it is now” and it does it frustratingly fast so I don’t have much time to try and avoid the permanent impacts (and there is little that can be done about physiological behaviours that happen automatically). My doctors and I know this from my medical history which includes stuff like… the injury in my right knee spreading to my left knee in only a couple of weeks (the start of CRPS). The IBS set in within a couple of weeks of the disruption. The respiratory issues were locked in as the new default within a week or two of being prescribed an incorrect asthma inhaler. These are just a few examples of how quickly new patterns become permanent in my body.
So here’s the Thing:
Knowing this about my body: if I were to catch the pandemic virus, even if I avoid fatal inflammation increase, I would have to absolutely get rid of aaaall symptoms within 1 week, maybe 1.5 at most, to avoid having to live with those symptoms for the rest of my life. I’m not being precious. I’m not a hypochondriac. I’m a scientist with a sucky disease. That’s it. It’s simple and it’s crappy. It is what it is though, and I don’t get to pretend otherwise because the risks are unbearable.
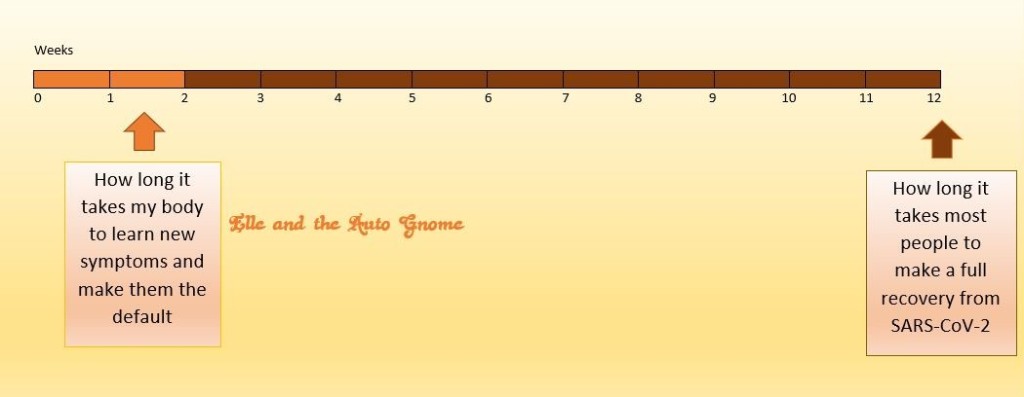
Most people make a full recovery in, wait for it….12 weeks!9 I know, right?!
12 week timeline with an arrow pointing at 12 weeks and the caption “How long it takes most people to make a full recovery from SARS-CoV-2” and then another arrow pointing at 1.5 weeks with the caption “How long it takes my body to learn new symptoms and make them the new default”
I literally can’t afford to catch it.
At all.
If I do, either I die or I survive but whatever symptoms I experience are incredibly likely to become permanent.
Imagine having COVID symptoms every second of every day and night for the rest of your life.
This is what I’m trying to avoid. Well, and dying. I’d like to avoid that for a while longer too of course.
I didn’t fully comprehend the severity of my chronic inflammation until a recent appointment, but I’ve tried to convey the lifetime-of-Covid-symptoms on multiple occasions. Many times I’ve thought I successfully conveyed this situation, my partner likewise, and then the next conversation or visit we’re right back to being invited indoors, being told we don’t have to wear masks etc and we’re glancing at each other in confusion trying to figure out what happened.
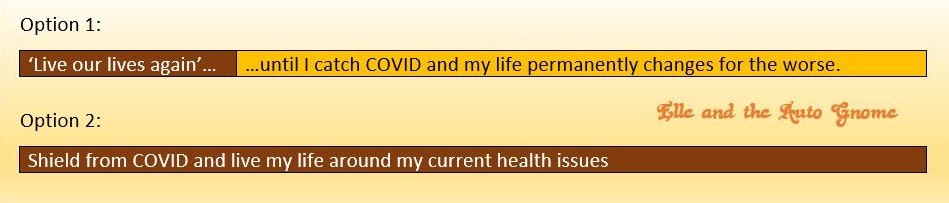
We still get asked: ‘when are you going to live your lives again?’ The last time we were asked this my partner replied that we could live our lives up until I catch covid and then we wouldn’t have that life to live any more. He said that at that point my life as I know it would effectively be over. Which is why we’re trying to avoid that.
Option 1: ‘live our lives again’…until I catch COVID and my life permanently changes for the worse. Option 2: Shield from COVID and live my life around my current health issues.
This is what so many fellow patients are experiencing right now. That dissonant horror of knowing that our loved ones care about us whilst experiencing them actively trying to dismiss our medical reality and repeatedly put us at risk. It’s obviously not what they think they are doing, they presumably think there is no greater risk for us, but why that view never changes no matter how many times we try to convey our reality is hard to figure out. It’s emotionally exhausting having to repeatedly explain that we are trying to avoid worsening our condition, getting hospitalised, dying or ending up with COVID symptoms for the rest of our lives. It’s so painful and upsetting to repeatedly be told ‘it’s no big deal’. They’re effectively saying they don’t want to protect us, and that is so very painful, but it’s often because they don’t realise our risks are so great or, worse, genuine.
There are some variables I can’t control. My partner is a keyworker but he’s also my carer. He does the best he can to protect himself and reduce the risk of bringing it home. His employers have no interest in protecting his at-risk partner and his experience is that the general public were about 50% unmasked around him while he’s working when the rules changed in July and he’s found that the number of unmasked members of the public around him has been increasing ever since. This already creates a percentage of risk for me and it’s already too much risk10 because I have to avoid catching it at all.
In my case a part of my brain is dysfunctional and detrimentally impacts my other body systems including the immune system. I’m an example of someone who ‘looks’ okay (because I rest and prepare before visiting / being visited) but whose condition is complex and multi-systemic. Many patients have more readily accepted situations, such as transplant patients and cancer treatment patients whose immune systems are, at the least, heavily compromised and yet even they are put at risk because people can’t ‘tell’ who is vulnerable by looking at them and tend to assume those around them have the same risk levels as themselves. There is a whole spectrum of conditions affected where patients struggle to explain the realities of their complex risk situation. So just because someone has a pain or other neurological condition, for example, does not automatically mean that their immune system is unaffected. Our body systems talk to each other and, over a chronic length of time, many other systems can and do become compromised. It doesn’t mean that they are ‘safe’ or that you or they being vaccinated will protect them enough to mitigate risks. The risk depends on the dysfunction within each person’s body and that isn’t visibly apparent.
I have friends around the world in my beautiful, knowledgeable, international patient network who also happen to be trained professionals with amazing skills11. We’re extremely well informed and continue to seek out the latest research, apply our skills to that and share the most reliable and useful aspects. Some of those friends have seen their risk factor become reality. For example, a friend with both CRPS and Dysautonomia now diagnosed with ‘Long Covid’ has extremely exacerbated autonomic issues that are impacting their life massively, (dysautonomia is also a commonly new condition in many previously healthy Long Covid patients9). Some friends with chronic CRPS have been told unequivocally by their doctors that if they contract the virus it would be astonishing if they didn’t die, and on the flip side an incredibly healthy and active friend seemed to be recovering from the virus when they went downhill and ended up rushed into hospital for worsening respiratory issues. Any of these scenarios could be me.
What can you do now that you know the risks are real? The main thing is to be aware of what poses risk and avoid passing that on to the patient. If you do not come into contact with the patient they are protected but if you are doing higher risk things and then coming into contact with them, or worse – living in the same house as them, you need to be aware of how those actions are increasing their medical risk. For example, my lovely partner (the famed ‘Magic Dude’) misses going to concerts with his brother. They’ve been attending multiple concerts every year for many years and it’s a good way to example the varying risk level so I’ll use that as a comparison with his day to day work risk…
At work: Members of the public popping in and out of the building around him, less than half of them wearing masks so any unmasked infected people will be breathing out in his vicinity for however long it takes them to run their errand in the same room as him. The amount of time they are breathing out in his space is key so the quicker they are gone the lower the risk. A door to the outside is usually open so there is some air movement in a small space. When indoors he always wears a good quality mask that helps to reduce aerosol reaching his nose and mouth as well as protecting others in case he unknowingly has the virus (he knows all too well that anyone could be in contact with a vulnerable person and doesn’t want to risk others). The longer he has to remain in one room with people coming in and leaving their breath floating around the more the risk increases. It’s not like he’s wearing swimming goggles or anything – if the virus comes into contact with his hands, face or eyes he is much more likely to bring it home to me.
At a concert: People in the same space for several hours instead of minutes increases the risk significantly. People shouting/cheering/singing loudly expells more aerosol than just breathing / talking, so this significantly increases risk as well. Even if less than half of the audience were wearing their masks (same percentage as at work) the risk of exposure to the virus is hugely increased. Even with my partner wearing his high quality mask there is a much higher potential for aerosol virus in the air and therefore of it coming into contact with him. It’s in a larger space but the air ventilation is poorer overall which also increases risk.
Another way of demonstrating risk is to flip the scenario: people running their errands around him at work don’t hang around for a few hours cheering him on wildly and yelling along with whatever tune he might be humming at the time. It’s a biiiig difference!
A line drawing of a man looking surprised, he is wearing a mask and holding a ‘To Do’ list. He is surrounded by several people waving, cheering and singing loudly.
Even an outdoor festival in Cornwall last month where as many precautions were set in place as possible, including testing people and refusing 450 of them entry as there was a chance of them carrying the virus…has still resulted in a massive surge of (nearly 5,000) new cases12. So we can see that even outdoor concerts significantly increase risk because of the close contact with others.
So once you know what puts them in more danger you can avoid those scenarios. The phrase ‘we’ve got to live our lives again’ is repeated regularly in the media and used sometimes as an excuse for putting others at risk. Living our lives again as we used to puts other people’s lives at risk. That’s just the sad fact of this situation we’re all in. Living our lives again with care about how we do so is the best all round way forward, especially for anyone in your life that you care about who is at greater risk.
Mitigating riskwhen you are in their vicinity If you have a loved one who is at risk then there are ways you can help protect them as well as ways you can help them cope with that reality too.
First and foremost, know that their situation is majorly different from that of people with fully functional immune systems. What is lower risk for vaccinated immune-tastic folks is still life-threatening for us lot. The first biggest difference you can make is to not just listen but to truly hear what they are saying. What they are saying is entirely appropriate and proportionate to their level of risk, which is simultaneously completely different from your level of risk from the same thing.
So let them know you’ve heard them and that you have truly taken the information in.
Then: behave in accordance with what you’ve said.
The most painful experience for us right now is people telling us that they ‘get it’ and want to protect us but then demonstrating the exact opposite with their behaviour and expectations. You’ve learned that they are at high risk so please don’t then put them at more risk.
You can do this by:
– staying away from them if you are unable, or not prepared, to take precautions to protect them. You could have the virus with no symptoms and anything you breathe out near to them or in the same room as them can come into contact with them.
– showering and changing clothes after being in the vicinity of other people before you go anywhere near them.
– still keeping social distance from them even if you are taking precautions to protect them. No precautions will fully protect them, so the more precautions you take the more you reduce their risk.
– wearing a mask anywhere near them and especially when in the same room as them. If you unknowingly have the virus a mask reduces the amount of aerosol droplets getting into the space around them10.
– opening windows so that there is an airflow through the room taking aerosol droplets with it. This is important because the viral aerosol stays in the air for much longer than originally thought, and it doesn’t leave the room with you once it’s in the air. Leaving virus droplets in the air of a vulnerable person’s room becomes a higher risk because the longer it’s in the room with them the greater the chance that it will connect with them. One open window only reduces risk a bit, two windows reduces it further and so on. The more airflow there is the lower the risk. One window open will stir it up a bit but won’t be anywhere as effective at removing it from the room10.
– if airflow is tricky there are ways to increase it without knocking new holes in the wall for more windows. Air filters with an effective aerosol HEPA filter will help remove viral aerosol from the air, though it is obviously better if it doesn’t get into the air around a vulnerable person in the first place. Some air filters also have ionisers which are effective at removing aerosol from the air. Just be aware that there is a certain amount of ozone byproduct from ionisers. Low amounts of ozone from air filtering devices are often acceptable but check it out first and with regards to the patient’s and your own health vulnerabilities as it is a toxic gas. If in doubt open a window for ventilation. This may seem backwards when filtering air, but it’s not if your aim is to minimise viral risk in a room. If you have an air filter with different settings you should be able to turn the ioniser off whenever you need/want to whilst the air filtration continues.
– meeting outside is far safer than indoors even with windows and doors open, but still keep social distance as this is key to keeping the air around them as free of aerosol as possible and think about whether the wind direction is carrying it towards or away from them.
It’s not just about the people you’ve met with, but the people they’ve met with, and so on Many people underestimate that the risk of catching the virus from anyone you’ve been near and then carrying the virus to someone else, but massively overlook the huge increase in risk when you meet anyone who has been in contact with other people. For example, one of our allotment neighbours was talking about only mixing with his “bubble” of people but was surprised to realise that the bubble isn’t actually a thing if anyone in the bubble is interacting with anyone outside of it. The bubble is only a thing if the people in it only interact with each other. Once anyone from that bubble starts interacting with others outside of it (meeting up with friends, going to school or work etc) they expose everyone inside the bubble to all the people they’ve been meeting (and all the people that those people have been meeting…) even though you haven’t. If any of them have the virus, that person is bringing the risk to you and when you meet up with anyone else you are then taking that risk to them. Worse still if you take that risk to someone for whom that risk is far greater.
Our eldest niece made an excellent example of understanding this when she went to visit her grandparents during the last lockdown. She refused to step inside their house and only talked to them from outside. They didn’t realise she was doing the entirely appropriate thing, but that didn’t matter because her choice of behaviour is what was important. She knew she’d been mixing with other people, she knew that having no symptoms is a Thing, so she knew she could be putting them at risk – and she chose to take precautions to reduce their risk.
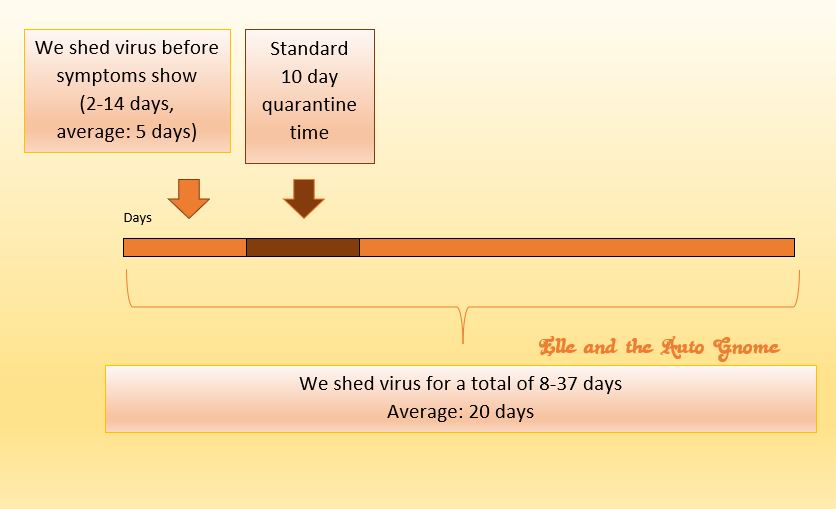
It’s suggested that the only way to avoid having to take those precautions is to quarantine for the standard 10 days13before meeting someone vulnerable as there is always the possibility of you having the virus with no symptoms. Every time you meet with someone who’s been meeting with other people your quarantine is broken and you’d have to start again as there has been another chance you may have been in contact with the virus. You are not ‘safe’ for a vulnerable patient to be with. However… even after quarantining there is still the chance that you have it but are assymptomatic (i.e. do not develop symptoms) because you can shed virus for up to 37 days14.
Timeline in days showing that we shed virus before symptoms show (2-14 days, average: 5 days)15 and for a total of 8-37 days (average: 20 days)14. The standard 10 day quarantine time only protects others for a part of the time we are shedding virus.
You can take a lateral flow test (currently available free15)which gives you an idea but that also isn’t absolutely definitive so please do still take precautions with anyone you need to / want to protect.
Vaccines in the general population Anyone who has had (and not everyone can or should have) the vaccinations has a reduced chance of both hospitalisation and death. So yes, vaccinated people can still catch the virus and although for most people the risks are far reduced, for some people hospitalisation and even death can and will continue to happen because the vaccine can only teach the immune system how to deal with it, how well your immune system actually does that will be unique to you and your immune system.
So…
– Being vaccinated does not mean that you are safe to be around. If you’re vaccinated you can catch the virus and pass it on to a vulnerable person or to their partner/carer/parent/child etc who would then take the virus home with them. Vaccination reduces risk to that individual but does not prevent infection or transmission17.
– New virus strains may not be as mitigated by the existing vaccines. Earlier information noted the effectiveness of the vaccines against the Delta variant18but it has since been found that the Delta variant is twice as contagious as previous strains19and two studies have suggested the severity is more likely to cause hospitalisation19. Fully vaccinated people shed just as much Delta variant virus as unvaccinated people20. The shedding of that variant virus doesn’t last as long as with other variants19but this knowledge isn’t helpful in practical terms as we usually don’t know when we’re shedding virus anyway because….
– Not having any symptoms does not mean that you are safe to be around. You can be infected and not know it because the virus sheds long before symptoms show. The virus can also present assymptomatically in some people meaning that symptoms never show up at all.
So being vaccinated and feeling fine / not having any symptoms is irrelevant to whether you are safe to be around.
Being vaccinated protects you from hospitalisation and death to varying degrees per individual but it does also reduce transmission in some variants to some extent (although the delta variant is virtually just as transmissable by people whether they’ve been vaccinated or not)19 – so it is a factor in helping to reduce the risk you put others at…. but…… you can still infect them and for vulnerable patients their risk remains about as high as it was before you were vaccinated.
By the way, symptoms in the vaccinated are generally much more low-key than in the non-vaccinated. You can see a list here.
Vaccines in the chronically ill Those of us in the chronically ill population who are vulnerable to the pandemic virus have compromised immune systems. For some of us our immune system is dysfunctional / compromised / entirely absent, for others our immune system is dysfunctional because of other health issues having that knock-on effect. Patients with compromised immune systems can sometimes still be safe candidates for the vaccine, but…
– If a vulnerable person has been vaccinated it does not mean that they will be safe around the virus. Those of us vulnerable patients who are able to be vaccinated are not as well protected by the vaccine from hospitalisation and death. As our immune systems are compromised they can’t learn as much from the vaccine or put as much into responding to the virus as a healthy system would.
We have all tried explaining this to our loved ones in the hope that they would want to help to protect us but it doesn’t work out that way. It’s hard to understand why because we’re coming from two completely different points of view and experiences. It’s tough to bridge a gap of misunderstanding when we don’t really get why the misunderstanding keeps persisting. We don’t know where we’re going wrong. On either side of the puzzle.
I really hope that this helps start to bridge that gap. If sharing this information helps people understand why their vulnerable loved ones are vulnerable then I will be immensely grateful to have been able to help in any way.
11. Our informal international network of patients who have professional skills and qualifications includes nurses, pharmacists, pharma reps, psychology grad’s, researchers, chemists….and on and on… CRPS, dysautonomia etc don’t care what we’re trained in, it’s happened to lots of us and we apply our skills usefully wherever we can
I just found out that my pal (also living with decades of CRPS) also hears screaming in her head. Whilst our outer presentation is calm and in control our inner voices are busy doing what we can’t do in the outer world. If we started it’d steal all our energy, undermine our steely determination and, frankly, we’d never stop because the pain never does. The inner screaming is the tell-tale of relentless suffering that our behaviour to those around us belies.
My pal and I work well together. Where my brain now fails, hers can handle it, and vice versa. Together we can get the job done because the bits that stall each of us are picked up and dealt with by the other.
The 1st sketch is of two women with their heads down on their separate desks, arms hanging straight down by their sides; an arrow leads to the 2nd sketch which is of the same two women sat at a laptop behind the same table smiling.
We chatted about the inner screaming and bounced ideas around. Her with her medical training and neurogeekery, me with my psych background and experiential approach.
Just because we have inner screaming doesn’t mean other pain patients do, but what if we all have something happening around the point (and beyond) that our body’s coping system goes into overdrive? Not the one where people notice we’re really symptomatic (because most people won’t see our pain until we’re on the verge of requiring hospital treatment) but the point where our inner alert goes off. Like one of those secret alarms that let the security and sort-stuff-staff know that there are threats that need to be dealt with. A message just for us, about the state our body is in.
What could it be for others?
Screaming is what my pal refers to as a primal response. That’s our clue. Primal. Nothing sophisticated – it’s not a chatty message, it’s an alarm going off about the unbearable. But the unbearable is our permanent condition. It varies in intensity but never goes away. This alarm could vary too. Be it inner screaming, nausea, physical shutdown/freeze, and such like.
Hardly surprising, as many years of chronic pain impact on all the internal systems that both talk to and inform each other. We develop lots of comorbidities in the same system as our original ‘fault’, but also in the other systems that are informed by the faulty system either directly or via the brain, or by a faulty brain that’s causing the original faulty system. In a nutshell – the human body communicates so thoroughly with itself to function, that a dysfunction does not get cordoned off or contained. It has multiple effects that accumulate over time. Alarm messages showing up in different systems is not a surprising outcome. Especially the longer the patient’s body has been dealing with the chronic pain.
Do you experience something like this? A marker of pain intensity that doesn’t necessarily involve pain itself? And all the while our exterior belies the extreme experience we’re living because it often doesn’t show on our faces as a ‘pained’ expression, or in our composure as a ‘pained’ posture or pain-impacted speech etc. We’ve had years, many of us have had decades, of having no choice but to live with the pain and as such it does not ‘show’ in the way others might expect.
Even
When
We
Are
Screaming
On the inside.
– It. Does. Not. Show.
A sketch of a woman with no expression (other than maybe her eyebrows are a little raised, I’m not the best artist, hehe), inside her head is a sketch of the person screaming in that famous painting ‘The Scream’ by Edvard Munch.. mouth open wide, hands to their cheeks, and zig-zagging lines radiating out from their mouth. Next to the sketch it says “Best ‘poker face’ ever…?!” and is signed “Elle and the Auto Gnome”
Interestingly, it can be calmed down. Sometimes noticeably so. It’s not a fix, it’s one tool of many we use to try and cope with what is a never-ending “ALERT ALERT ALERT” situation inside our bodies.
I’ve been learning this year how important it is for my health that I make sure I take time for me. Specifically time to do something that makes me happy, that I enjoy, that feeds my soul or my hunger for knowledge. Something literally just for me. After trying to factor it in because it had dawned on me (fiiinally) how much I am skewed towards trying to be ‘useful’ or ‘productive’ I then also discovered that it really helps me to stabilise symptoms and improve my baseline pain and functionality whilst reducing my stress levels. I know. It’s obvious to everyone but us, right?! But the internalised ableist Guilt of not being “productive” in the way our society frames it means that it is absolutely commonplace for us chronically ill patients to disallow ourselves any fun or relaxation because we have not been productive enough and don’t ‘deserve’ it. And if we do allow ourselves time the guilt eats away at us.
Today my visiting CRPSer pal has been reading a book for a prolonged period of time whereas audiobooks are usually the only viable option for her. Turns out the calm friendly company has quietened the screaming which is allowing her the option of either for once. Nice! Mindfulness is all well and good but it’s blooming hard work when there’s inner screaming or it’s equivalent. What is making it easier for her is being in the company of someone she feels relaxed and comfortable with instead of battling the pain alone.
There’s all sorts of research about how our loved ones impact on our experiences and it has been notable how research participants can endure significantly more pain when in the company of a loved one, in fact, even with just a picture of them to look at! Many a time I’ve commented on how much better I can cope when Magic Dude gets home from work. He’s not just a distraction, he’s not just someone who brings me food, fluids and hot water bottles to save me from making my symptoms worse trying to get them myself… he makes me feeeeeel better. His existence helps me cope. Preferably his close proximity but even chatting to him on the phone when he’s on his work lunch break can have a significant effect. It’s not just partners of course, it’s people we love. They might be family by blood, family by soul and heart, they might be furry four-legged family members…love helps, but is it really the love making the difference? I feel that a significant part of it for us painees is the external focus on that person or on that love. We are trapped in these bodies with the pain and the screaming and the dizziness and the lack of functionality….an external focus that we love is a handy option in our toolkit.
That would mean though that it doesn’t have to be a person, whether a human or animal one. Indeed, many of us have creative hobbies which, despite taking a physical toll of some sort, we love and persist with. Whilst we’re drawing / colouring / sewing / designing / writing / taking photos / crocheting etc our heart soars with the joy of doing something we love. Engaging more strongly with a focus outside of our tortured internal experience doesn’t change the inner experience, but it does tip the seesaw of attention in a more bearable, even enjoyable, direction.
It doesn’t stop the pain; it doesn’t solve the problem but it can help us to cope. Calm that silent alarm down for a while. Give us some hint of respite from the pain that never ever relents. Allow our nervous systems to dial down the alert level so that our systems can run at lower levels of horrific for a bit. It gives our bodies reduction in the intense stress and strain on our systems that is otherwise non-stop high-level impact. Enabling us and our internal systems to rebalance and restabilise to some extent – and that is crucial.
So, to temper the silent alarm we have to do more than just manage our health. We have to acknowledge ourselves as more than just a patient with health needs and allow ourselves to feed our hearts and souls. Often an external focus can help a bit, whether it’s human, animal or hobby. Whatever helps, right?
Ridiculous that having performed and taught Tai Chi I should be so ridiculously unbalanced in my lifestyle approach eh?! It’s so hard to see it when we’re in it though. And ableist views of productivity and usefulness are so ingrained in us that it takes a good while to work them out of our psyche and reframe ourselves more appropriately and realistically.
The 1st sketch is of a woman’s face with open rounded eyes, her thought bubble says “I must try to be useful aaall the tiiime”; there is an arrow to the 2nd sketch which is of a smiling woman, the writing next to her says “OMG! I function better if I take time out? Whuuut?”
So if it helps, here’s the Thing:
Moments of enjoyment and relaxation are not something to feel guilty about because…
…they are in fact a crucial part of our pain and health management that we must not neglect because our systems are under such relentless continuous stress that it is imperative that we do so. We have to factor this into our daily lives along with our other management tools.
So you don’t just have permission, it is a necessity.
We’re both interested in your experiences with this and realise that our different writing styles make our conversation accessible to different readers. Plus I was intrigued to find out how differently my brain would write about the same subject considering that she and I work really well together because we come at things from different angles and with different approaches. Heh, you’d think I was trained in research or summat! 😉 (Spoiler, I am, heee).
I did a little chat to video for my healthy, mostly able-bodied friends because crips like me are old hands at handling isolation so we can share some tips that might help. [Hmmm, Tips from Crips, maybe that should’ve been the title? Crip Tips?] Aaaanyway, then my friends all asked to share it so here it is in written form because the audio was not always that clear…
.
Admittedly it’s initially been hard to deal with the healthy folk not coping with their, what is to us, very brief and temporary isolation with their mostly functional bodies. We’ve continued at the periphery being referred to as ‘other’ through the “only” the vulnerable will die phase, then people buying everything leaving the vulnerable without, then people not staying at home to protect the vulnerable and finally only doing so when it seemed to be important to them personally and now they are at home and we’re finally being risked less – we’re hearing a lot of complaining about how awful it is being stuck at home temporarily whilst able-bodied.
And I’ve shared about this for insight because healthy people can look at their current experience and try to imagine what that’s like as a forever situation because that could mean more awareness and care for people like us out on the periphery, but what I don’t want is for people to feel shamed into hiding their frustrations because ‘so-and-so has it worse’, that’s not helpful at all. Your frustrations are valid, even though we’re jealous of you because even in lockdown you are capable of all the things we would like to do at home but either struggle to do at all or simply can’t.
When life gets harder, you must have just leveled up!
But we do have a lot of experience dealing with isolation so…
First of all – yes, being stuck at home sucks. The early stages are particularly potent as we go from living a faster paced life to what feels like a standstill. Over time you’ll settle into it more but let’s see if we, the long isolated chronically ill lot, can help with that transition at all.
Not all of our experiences are relevant to you. When we first found ourselves where you are we had lost our identity because we could no longer work (amongst all the other things we could no longer do) but what we do for a living is key because that is how we’ve been raised to define ourselves. The standard “and what do you do?” question that we get all the time because the assumption is that everyone does something, and we do, but what we do doesn’t ‘count’, as it were. Even after no longer being able to train for a career, work to earn an income, do the things we used to do and go out to see friends, go on excursions, to events etc we still don’t actually do “nothing”. Our time is filled with pain and symptoms and finding ways to cope with that on top of the frustrations of not being able to do stuff. So we will spend hours trying to build our body up to trying to get some food, trying to have a shower etc.
This is obviously not how your time is being filled. You are mostly able-bodied, used to being on the go and suddenly find yourself stuck indoors. You’re most likely really frustrated and because you can’t go out you and we’re all only human, you are probably wanting to do all the things that involve going out.
So here’s the trick, and when we (the chronically ill) get told this initially it sounds really offensive until we understand it better but as you don’t have the health issues getting in the way it might make more sense to you earlier on…the trick is… “acceptance”. <shudder>
Yes it sucks. We haaaate this one! But the key is that this is not about ‘giving in’, not at all, it’s simply about acknowledging the parameters of the situation because once we’ve done that we stop bashing our heads against them and are freed up to think about what we can do within those, admittedly sucky, crappy, horrid parameters.
So…seeing as you’re stuck indoors, what is there indoors that you could do?
Yes, all the cleaning and DIY etc
But, also
Who are you? What do you enjoy? What have you been putting off or not getting round to that you’d like to do or try? Not work related stuff. You related stuff.
Who were you before the adulting?
Art? Books? Writing?
This is your time. To be you. Indulge in yourself.
We try to do this but it’s hard because we mostly still struggle to do any of this stuff. Managing to get to the toilet has to come before doing something for us. And doing something for us always renders us in more pain/with more symptoms etc so it ends up being a rare thing indeed, but you have this opportunity here because you’re not restricted like we are. I’m not saying ‘ooh look we’re worse off than you’, what I’m trying to say is… you have the opportunity to really run with this in ways that we can’t. This could be pretty awesome!
At first it kinda feels like you’re at school and have been told it’s ‘indoor play’, ugh!
The trick is to re-frame it – it’s not so much like indoor play – as getting to go home early! You can play, it’s guilt-free time to just ‘be’. And you can do it in your house with all your stuff. So be you.
No-one else will see… your drawing, your poetry, your writing, your new attempts at recipes with the random ingredients you’re having to work with! No-one will see your home-made videos (unless you choose to share any of these afterwards of course). No-one will see your fort (oh yes, adults can totally make forts too). The decision is all yours.
One key tool that we use is not to look too far ahead into the future. So rather than looking at the potential weeks at home stretching out ahead of you the trick is to think of a thing you’d like to do and focus on that instead. We rarely know what day of the week it is because unless we have a doctors appointment they are basically the same Groundhog Day over and over. If we acknowledged the days going by without us we’d be a forlorn mess. All those people living their lives when we no longer can. In this instance though you’re not getting left behind because everyone is in the same boat. Or most people anyway. Most people are having to isolate and not do what they usually would be doing. So you have an opportunity to play without getting left behind.
Re-focusing helps with worries about the future as well. Income is a concern for many. We understand this concern, it is ever present in our lives and unless we could step back from that we would never cope. We don’t just block it out, what we do is what we can for now – get that set in place. Then what is out of our hands is out of our hands. Worrying about it would send us doolally with the stress about the resulting impacts that would bring. So once we know we’ve done all we can for now, we step away from that as well and consciously focus on something else. For our own sanity. This is crucial. Do what we can then shift focus.
Stopping to notice the little things. People don’t usually do this unless they’re are on holiday. It takes some time to wind down and slow down enough to do this. Work on it. Have a cup of tea, look out of the window, notice the sounds, the feels, acknowledge anything that you like. Let it make you smile. These little things pass us by usually but when we’re isolated they become a quality part of our lives.
Keep in contact with others. You’re used to seeing people every day and suddenly it’s not happening. The silence can be deafening. Check in with friends. Send messages, silly pics, make video calls, have a laugh. Contact friends who live alone or are chronically ill, the former are currently extra isolated and the latter are always isolated and are suffering from years of this. You will make their day just by saying hi. Trust me!
Keep some semblance of routine though so that your body doesn’t rebel too much. Sitting around in jammies all day is okay for the first couple of days but then we really need a focus or things can easily slide. If they do that you can find yourself without a coherent sleep cycle or decent nutrition and if you do get ill your body may not be so ready to deal with it. So keep clean and get dressed, have mealtimes still, look after your body and be you.
So to re-cap, some tools we use:
Accept the parameters (they’re shit, we don’t get to choose them)
Re-frame it as an opportunity
Don’t look to far into the future: prepare as much as you can for eventualities and then re-focus
Get in touch with who you are on the inside, regardless of job, positions in society etc
Look for possibilities within those parameters that might make you smile
Take time to pause and notice the little things
Keep in contact with others (we have the technology)!
Keep a routine so that your body has enough sleep, nutrition, exercise etc
So…what do you feeeel like doing? What do you have in the house? Are you gonna put a tent up in the garden and listen to the birds? Are you gonna do some drawing in secret just for your heart’s content? Do you feel in need of putting on some music and having a really good dance-like-no-one’s-watching moment? Awesome! Do it! Not sure what your focus will be yet? No worries, stick the kettle on and have a think. That’s part of the process. Rediscover who you are on the inside and allow them out to play. You might find one thing you want to do or you might find lots of little things along the way. You might prefer to make gifts for other people to make them smile. It’s all good. Let your inner you take you on an adventure.
I wrote this the other day and it’s very rough around the edges but as this is a window on current events I’m posting this during the time it’s happening. Here is why The Spoonies are Baffled…!
.
The stuff healthy people have been panicking about has seemed kinda surreal to us Spoonies. It’s just so far from our reality. That’s not to say their concerns are less valid than our own, everyone’s concerns are valid, but they can be very different indeed and from a broader view there is a distinct difference in scale of risk e.g. ‘I’m worried I might run out of food’ on the one hand and on the other ‘I’m worried about my heightened risk of death, I need to isolate for my own protection but am having to go to the shops even more than usual to try to find food because everyone else seems to have bought it all’.
A cartoon sketch of me looking utterly perplexed.
Magic Dude is having to come home via the supermarket more often, not less, because he has to keep checking if the essentials that weren’t there have been re-stocked yet. This is the complete opposite of what he should be doing as he has a vulnerable partner at home. We live in an individualistic society, I know everyone looks after themselves first, but buying up all the supplies so that the most vulnerable can’t isolate feels pretty personal when you’re one of the ones being put at greater risk.
Healthy people will have to be at home for awhile. Anyone who does this will save lives. We generally cannot do all the things that you can do at home. To us you have a superpower, a privilege of relative health and able-bodiedness. You have time at home during which you can do stuff that we battle our bodies to do once in a blue moon.
Seeing as our worst case scenario from catching SARS Co-V2 is death… running out of loo roll is pretty meh to be honest. We have cloths and a washing machine. I’d rather that than die. No biggee, right? Stuck at home for a few weeks, meh, try decades, we’ve got this! Having to explain to people why they shouldn’t put others at risk, weeell that’s an extension of endlessly having to explain our conditions anyway, we even have to explain our specialist conditions to non-specialist doctors so it’s basically same-old same-old. But none of these are easy. Having no toilet roll is, well, shit! But more so when you’re chronically ill and less able to do washing. Being stuck at home but being unable to do anything owing to the chronic illness is sucky beyond description. Having to explain why we have a right to treatment/life is indescribably exhausting and demoralising. But when my bruv called me the other day and asked how the lockdown was going I said “same as always!” and laughed, because this is my life. It’s not going to pass. Everyone else will go back to the Great Outdoors and Doing Stuff and we will be left living our lives silently behind closed doors again. Forgotten about once more.
A lot the stuff healthy people are currently worried about and experiencing to a lesser extent, for the most part, also creates a chance that maybe, just maybe, some people will get an insight into how they are aspects of our permanent,daily lives.
An ‘ah-ha moment’ could potentially happen!
How long they’ll remember that is a whole ‘nother thing, but still… a moment of understanding from people usually outside of comprehending our reality can be important. It can strengthen or recreate a connection to those friends who don’t really keep in contact, who don’t visit even though they always say they want to, (a typical impact of chronic illness is loss of friends and occasional empty promises of seeing a 3D human are initially thrilling but often ultimately devastating). We’re so isolated pretty much all of the time.
For years.
We see doctors and sometimes family.
And.
That’s.
It.
Each year I can count the exceptions to this rule on one hand and still have fingers free to hold several biscuits at once. (This may of course be a bonus)?
So yeah, this is kinda like my experience growing up in the countryside and getting snowed in by 6’ snowdrifts a couple of weeks per year, then moving to a city and witnessing the carnage and panic caused by a mere dusting of snow. It was so beyond my comprehension that anyone would act that way in what, to me, were such minor circumstances that it was truly surreal to behold! The chronically ill community and our carers are seeing the healthy population do things that we find utterly bemusing under the circumstances. Magic Dude has often been lost for words to describe his befuddlement over what he’s been seeing and experiencing when he goes on essential food runs. There’s talk amongst healthy people of how it’s not surprising because people are under so much stress, and yet we’re still utterly bemused because we are under at least that much stress all the time and we can’t comprehend how it would cause that behaviour. To us it looks like a madness of sorts.
Then there’s the angering behaviour. Some crafters have been smugly showing off their finds online as if there’s nothing wrong with buying the last bottles of alchohol swabbing stuff from the diabetics stock. Seriously? How is this acceptable in any shape or form? I can’t imagine what kind of people would see such a post and cheer at someone effectively saying “I can craft at the expense of a vulnerable person’s health. I did this by choice. Yay me, bet you’re so impressed/jealous!”? Or at least, I don’t want to imagine those kind of people. Or those moaning about how the vulnerable customer hours at supermarkets are filled with ‘normal’ people when, you know, invisible illness is the majority of chronic illness and these people are very vulnerable. We’re as invisible and deemed irrelevant as ever it seems. In the UK we had weeks of ‘oh it’s okay, only the elderly and chronically ill will die’. Oh. That’s okay then. (Arse).
So… we have to look out for each other because in our extensive experience pretty much no-one else is going to.
Fortunately, the UK is now catching up with what we knew was coming weeks ago and did nothing about. The government has advised we remain at home and only go out for essentials such as procuring food or medicine. Magic Dude has fiiiinally found that places he’s getting sent to for work are no longer packed with people. He has been designated a ‘keyworker’ and can’t work from home so he can’t fully protect me (or himself, he has asthma) as he has to go out into the world and he has to come home to look after me. We need others to protect us by not going out there. Humans shed coronavirus for days before even starting to show any symptoms, so not feeling ill has no relevance to whether you are spreading the infection to vulnerable people. He was working in a hospital the other day and overheard someone say “I realise it’s real, now”.
<headdesk>
Meanwhile, here’s an insight to what’s been going on in the chronically ill community. First: it’s… well… a community, so it’s not so extremely individualistic because we strongly identify with each other. We’re part of the same tribe. Broadly speaking there is support and information being shared, a good support group can be invaluable to a patient. There are differences and personalities that clash but when the shit hits the fan we band together. Unlike in the healthy population the main go-to is not ‘save myself’ individualistic values. The main theme is information based – we want to share it to protect each other and the information is even more important to us because we are far more at risk from complications, but not everyone is trained on assessing source reliability. Sharing anything we see without checking the source is how unhelpful / incorrect information gets spread. This is an issue for healthy folk as well but a) it doesn’t risk their lives to the same extent and b) it seems to be secondary to Buying All the Things.
We know what it’s like to be without. To be restricted. To not have health support. To need meds and not be able to get them. The majority of help and information-sharing that I’ve seen in my social media network of both chronically ill and able-bodied has actually been from the chronically ill. Those who are most limited and most vulnerable are being most pro-active about protecting others. ‘At risk’ people still recovering from the coronavirus reaching out to share crucial information with fellow patients. ‘At risk’ people in hospital reaching out to their fellow patients because they know those are the people who understand the risks and complications and can offer relevant info or advice rather than empty encouragement. ‘At risk’ people sharing information to protect their at risk friends and extended family.
The other type of friend in my social media world who have been sharing valuable information are my science friends. Some friends are both ‘at risk’ and scientists. (Yes, we can be both highly qualified and intelligent while also being chronically ill and even cognitively impaired).
The general kinship of the chronically ill is often online because that’s where we live. Social isolation is nothing new to us, it has been our bane for years, often decades. For me, getting to a Tai Chi class was the most social event I got to go to. Since I deteriorated post-fall over 3 years ago my social gatherings are pretty much only with headphones and a laptop. We get to know each other, we get drawn to people who have the biggest overlap with us in a Venn diagram of who we are. Friendships are made and then this happens…
There are tight knit online networks of dear friends who’ve seen each other through thick and thin for yeeaars. Shared with each other details which we can’t share with our healthy friends coz the majority have enough trouble coping with what they know about our illnesses already. Risks of surgeries get discussed in reassuring but practical ways around the condition in question. Health hiccups get posted with questions and the ill-friend network answers. Research papers get shared to inform confused GPs. We can be honest about severity and risk factors because we ‘get it’, we aren’t phased by the severity of everyday issues because that’s our daily experience too. Severe and in-your-face-real is what we have been dealt by our conditions and fellow patients are best placed to understand and support each other even though we’re each up to our eyeballs already.
Along comes another threat to our health. Only this time it doesn’t just threaten one person in the group at a time, it threatens all of us at once. But other than that, it’s ‘just’ another threat to our health. Admittedly it’s a big one, but the point is that this is what we Do. This is what we live with. All the [hecking] time. The risks we face with our health, our treatments, our meds etc on a daily basis are constant and continuously fluctuating and morphing. So we’re not only having to deal with this continuously but also having to endlessly adapt and be flexible to the shifts and changes because they change the problems, complicate them, force us to learn more to understand the science so that we can explain it to our non-specialist doctors. If we don’t we’ll go under. We’d get taken down by the severity of our symptoms, our meds side-effects, our lack of treatment, our lack of medical support and/or understanding. It is relentless.
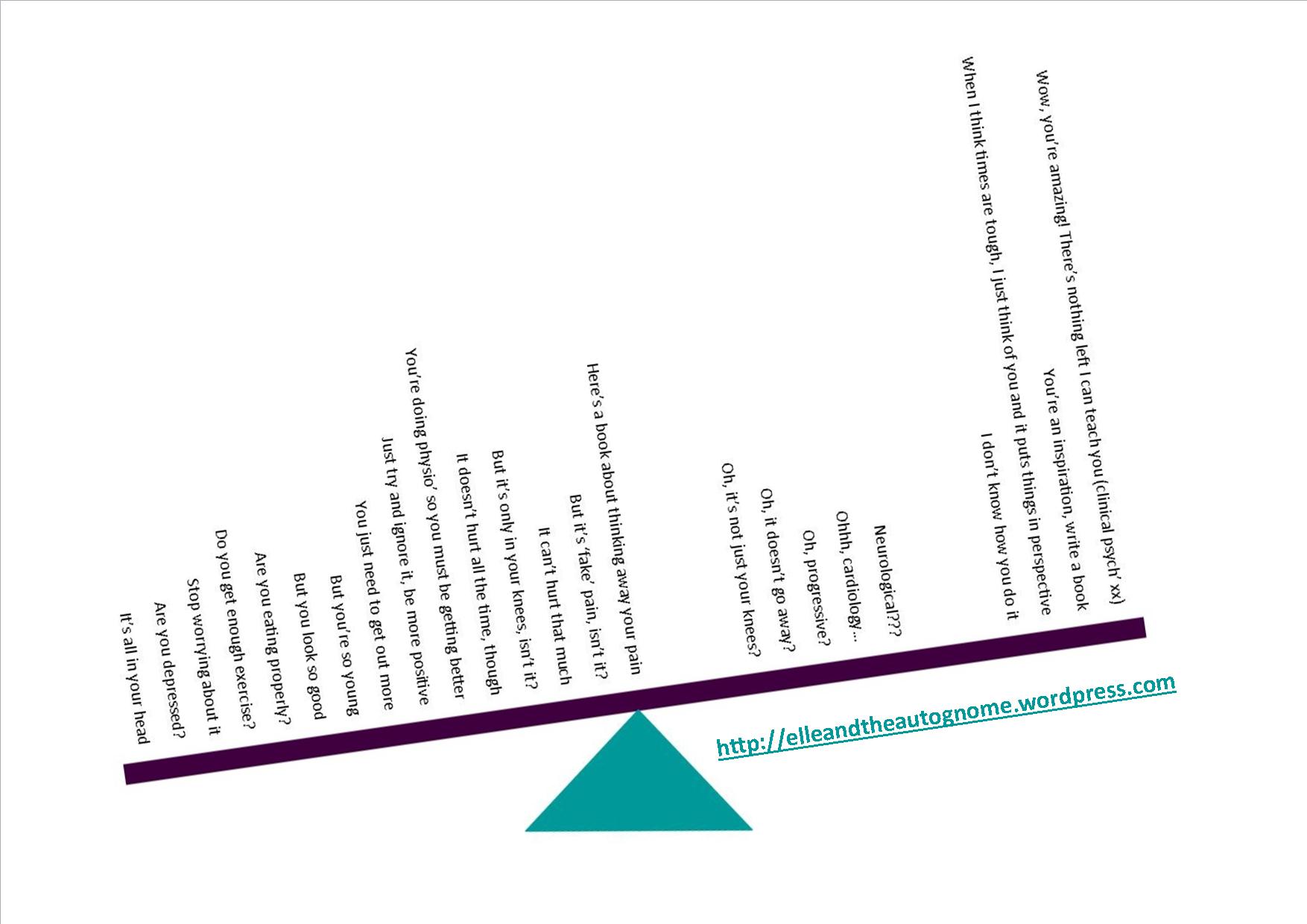
In light of this insight into the differing responses of the well and the ill, it is hardly surprising that there were initially memes all over the chronically ill community about how when the ‘normies’ are ill we should suggest thinking positive and trying yoga. This is amusing to us because….we get told that shit aaaall the time. Sometimes people will go out of their way to specifically write us a message about the wonders of [insert magical cure here]. Having to repeatedly point out that stuff that helps with certain issues to small extents cannot magic away a neurological condition gets old fast. So after all the yeeeaaars of getting this repeatedly from sooo many people…this is darkly amusing! It’s cathartic!
A seesaw diagram leaning down on the left of the fulcrum. On the right are a few postive comments from medical practitioners (including “There’s nothing left I can teach you”). Weighing it down on the left are a lot of uninformed and damaging comments from others e.g. “Here’s a book about thinking away your pain”, “You’re doing physio so you must be getting better” right through to ” It’s all in your head” on the far left.
And when people are complaining about getting bored at home we’d like to point out that we’re soooo happy if you’d like to swap awhile, you can manage this crap for a bit whilst we finally get to paint and DIY and garden and Tai Chi and bake and and and….all the things we could do at home if we only were well enough.
Of course we could resort to that other age old claptrap we get and start telling people that “it must be sooo niiiice to be at home aaall the tiiiiime”! (Spoiler: it isn’t). (Especially when you are ill and it’s forever).
We use humour to cope with yet another threat to our health (and potentially to our lives) because there are so many of these over the years that a somewhat dark and twisted humour becomes a survival tool of sorts. But what we really want is for no-one to ever say this crap to us again. That maybe they will get some insight to our lives through how much they hate having to stay at home for even such a short time, how bored they get when that’s not even a drop in the ocean yet. Or maybe, and here’s a thought, they might actually stop buying aaaall the Things.
Our healthy friends won’t ever truly know just how relentless that stuff is so they’ll never know how much of a relief it is when they don’t undermine our entire existence and everything we battle through 24/7 with one ignorant, offensive comment. But this health-scare experience might mean a few additional people realise how inappropriate that stuff is. Every little helps, right?! A few less comments like these to deal with would reduce the amount of daily crap we have to deal with. Which would be nice, right? So I can hope, right? (Magic Dude says my most annoying trait is how ridiculously optimistic I am, but I need it to survive so it’s staying).
We love our friends who don’t come out with the Stoopids. To them we say ‘thanks for not being dicks, we The Spoonies appreciate it!’. They’re probably the people who aren’t panic-buying everything from under us, too.
Maybe now that the reality of the threat is sinking in we might see a change in behaviour to something more sustainable to get us through the next few weeks or months. Over-burdened hospitals means that people with no virus but who need to be treated for car accident injuries or a heart attack, for example, may not get the treatment they usually would. Their risk of death is higher because having more critical patients than ventilators means that choices have to be made. Those more likely to survive will be the lucky ones prioritised for treatment. In other parts of Europe we are hearing from nurses openly saying that patient age is currently their first decision maker. Whilst this goes on everyone is at risk, not just those vulnerable to disease complications from the virus. And as people realise this they are finally staying indoors, because now it affects them instead of ‘just’ the vulnerable. <sigh>
As Terry Pratchett pointed out we can be pretty intelligent individually but get us in crowd mentality and we can be pretty stupid. Everyone for themselves and reacting en masse. We see a difference in the underdog groups though. By definition we need to come together to survive because as individuals we don’t count. And we do that as best we can in the face of whatever the masses are doing.
Those chronically ill patients that are also ill with potential COVID-19 are reaching out. Some are in hospital, some at home. Those of us that have any info on potential mitigating factors are sharing them, and there’s a whoooole lot of unconditional support between crip besties. It’s still not quite feeling like spring yet though and winter beats us up to a desperate symptomatic heap of non-functional. Many of our pals haven’t come out of winter shut-down yet, they’re still trying to get to a level where they feel they can communicate. We see posts from them before we get messages. If there’s posts we are reassured, when even those go quiet we know they’re having a ridiculously tough time. Suicidal thoughts are not uncommon for people living with such endlessly intense issues impacting on them, we are used to talking to each other about such stuff. I post stuff regularly and know that my pals are reassured by that. My healthy pals have a different concept about that than my fellow patient friends, they tend to see this as a sign that I’m ticking over okay or at least mostly coping. The latter group know how much I’m struggling not because I tell them more, but because their insight into the reality behind my posts is razor sharp as a result of their own experience. I’m not saying I get suicidal btw, I’ve been there and come through it by my own decision (those that have been revived by medics or talked out of it by others have a high risk of recurrence whereas I’m a stubborn old bint who made a Decision, damnit!) But I’m saying that it’s not uncommon for the chronically ill, and understandably so. And then the government and media declared that it’s okay, only the vulnerable will die. It’s okay. It’s only us. We have no value. No worth. And here’s that other uphill struggle. Where society says our value is in ‘what you do’ in society, for a living, to earn money. It’s bollocks of course, but it’s internalised and takes some (a lot of) routing out. We have to band together to acknowledge each other’s worth, lift each other up, encourage each other. “Keep going.” ” I’m here.” “You can do this.” and that gem of a friend who says “how can I help?” , listens to you turn down their help numerous times with very sensible reasons and then does their own well-informed damage assessment of your situation and, when required, says “tough, I’m helping you anyway!” We have to counterbalance the damage that general society does to us, by sidelining us when they’re not actively punishing us for being ill (I’m not getting into that here, but trust me, benefits assessments are not accurate, people who look ‘normal’ can have genuine need of a disabled parking bay, not being allowed to events because they haven’t made buildings accessible to everyone etc, it’s very restrictive and punitive for a group who are already being punished 24/7 by their own bodies)!
So yeah.
Suffice to say being chronically ill a) sucks, b) results in invisibility / disregard / exclusion and c) stop buying all the Things!
I need tea.
Anyone else fancy a cuppa? Kettle’s going on (when I can physically get to it) xx
Pencil sketch of me with crossed eyes determinedly trying to make tea. The thought bubble says “must…make…teeaa”.
Feeling hopeless and unmotivated…what the…? I always had the motivation to do my daily paced physio’. For yeeeaaars. It’s towards my quality of life through pain management so why wouldn’t I?
Brain chemistry may be part of the problem, though….
When we’re chronically ill we tend to get through a lot more neuro-chemicals than we used to. There are constant symptoms and sussing how to manage them as we go along – should I attempt this now or later? If I do it now then this, but if I do it later then this. If I take that med/supplement or eat some food or do that physio first then it will impact it like this or with those variables maybe like this. So I’m thinking maybe I should do this but with these provisos and that back-up and constantly monitor symptoms and be ready to adapt at any given moment as things pan out…. etc etc. There is a huuuuge amount of chemicals getting used up just trying to do the most basic of things. Then if we try to do anything other than the usual getting through the day stuff we decline faster and take longer to recover.
Back when I was studying I found that I will consistently lose my brain if I use it. Not the adage we more often hear of ‘use it or lose it’ eh? The more I use it (more time, more intensity, more challenge – any of those will do it) the quicker I’ll lose it and the longer it will be down for. My fellow CRPSer and blogger, Isy Aweigh, employed her nurse skills and suggested I need more dopamine to help my brain replace the neurochemicals I was using up. To create more dopamine, I need a source of phenylalanine. Us humans can’t make it internally, so we need it from food sources. I’m a veggie so meats are out, but aged cheeses are another source. And they helped. Significantly!
It’s several years later though and my neuro’ dysfunction has been telling my immune system to react to all sorts of things, one of which is cheese so that’s that one out of the window!
I was chatting with the same pal the other day about my uncharacteristic lack of motivation and overwhelming sense of hopelessness about how I simply can no longer Brain long enough to do the research work required to gain any useful health support from medical practitioners. Guess what I might need? Yup, dopamine! Seeing as I’m still a veggie (that’s not gonna change) and that I can no longer eat any solid cheeses I’m quite possibly deficient in the phenylalanine that I need to manufacture the required dopamine. It turns out there’s a supplement for it, who knew?!
After doing a quick bit of research (very quick, my brain falls over soooo fast these days) I found that the natural source found in foods is L-Phenylalanine. It’s not only used to make dopamine though, it’s also used to make other neurochemicals: adrenaline (epinephrine) and noradrenalin (norepinephrine) but it would be weird if balancing neurochemistry was easy, right?! We always need to consider all potential impacts and contra-indications (negative effects on med’s we already take) of any new med or supplement before we start taking it. In my case my ANS-balancer is an SNRI which inhibits the re-uptake of norepinephrine to reduce my flavour of dysautonomia. I was doing well on it until this potential phenylalanine shortage so rather than mucking up any previous balances, the supplement should (if it’s needed) return my neurochemicals to their happier levels.
There is also the artificially manufactured D-Phenylalanine which may well help with the production of dopamine as well, but it looks like the science isn’t completely in yet. It may help with pain however, and the side effects do not outbalance the potential for me personally so the standard mixed DL- supplement looks like it’s a Go.
Symptoms of a deficiency in phenylalanine pretty much describe my current state. Confusion – ohhhh yeah. Lack of energy – in the extreeeme. Decreased memory – significant, noticeable and upsettingly so. Diminished appetite – er, kinda, less appetite and depressed so I’ve been eating sugary stuff on hand and am now unable to fit into my shorts this summer. Possibly any summer. My first significant over-waistband roll. Oops.
I also found out that more than 5,000mg of DL-phenylalanine per day can cause nerve damage. Soooo I’ll be taking less than that then!
I ordered some DL Phenylalanine (a combination of the natural L- type and the manufactured mirror imaged D- type) from my usual reliable supplier of quality supplements and I’m gonna see if it helps me at all. Recommended is 1 x 500mg tablet per day. Not sure if that amount is gonna give me much Brain Time but it’s a place to start. I consulted one of my science whizz friends (fellow blogger the Hypermobile Hobbit) and she has raised a very important question – what’s the ratio of D- to L- in the supplement I have? Good point. L- would be more readily used by the body, so I’ve asked the supplier and am waiting to hear.
First, I figured I should list my current issues so that I can look at a before and after picture. Here we go, this is where I’m at:
Utter fatigue, all the time
No brain. Like, really no brain. I struggled to order two photo prints from the usual website we use. I managed two and then couldn’t understand the website anymore. Had to ask Magic Dude to take over.
When I’ve got no brain it kinda hurts. Sort of like a headache but different.
No idea what the heck is going on a lot of the time, can’t understand concepts, sentences, sometimes takes me awhile even to figure out the meaning of individual words.
Memory shot to pieces. Have got used to not remembering anything now. Whole events/days go missing. Previously I would randomly forget ever seeing entire films but it’s so much worse than that now. I even think of something like ‘I must tell Magic Dude this’ and instantly it goes – I have lost the thought less than a second after I had it and he’s sitting right theeeere, it’s not like I had to remember it for any longer than it takes to say it. Really distressing.
No motivation whatsoever. Just an overwhelming ‘it’s too hard to sustain’ and ‘what’s the frickin’ point, anyway?’
Endless migraine. Relentless. Can’t do anything that doesn’t send it soaring except for prop myself up on the sofa in front of the laptop raised on its over-my-legs stand and there’s very little I can do in that position because I mostly have no brain.
Want to bury myself in something creative but not enough brain to finish any of multiple blog posts I’ve started over time. Tried sewing and it’s great but it sends the migraine soaring so can only do that for a short while once a week or so if I’m lucky.
Lots and lots of physical health symptoms that are hard to grapple with but I’m not listing them here as that’s not the focus so much as how I’m dealing with them (or not). I’m down in the dumps about coccyx pain being permanent, about near-fainting all the ruddy time, about not being able to choose to do anything useful or anything nice/fun, about not being able to go to Tai Chi classes or even manage any at home since my fall injury a year and a half ago. Yeah, really really down for a long time now. Not like me at all but I’ve been avoiding everyone online because communication has become so hard. I’m on a veeeery long waiting list to see a neuro’ and trying to cope in the meantime. Coping isn’t viable so I’m aiming for ‘exisiting’. That’d be a win, right?
Being near fainty all the time means I’m not safe to drive. I can’t get out of the house at all. I am completely independence-free. I managed to drive round the corner to collect prescriptions a couple of times in the past year or so but it took all day to try to get my body functional enough for those few minutes of driving and then there’s the lengthy negative health impact of that to work through afterwards.
Coming up for 19 years with this neuro’ condition and this will be the first time I’ve *ever* been referred to see a neuro’ – see why us CRPSers feel so flipping hopeless at times? It’s hard bloody work trying to get basic care because wiring issues are barely even touched on in medical school. Plus – most neuro’s are brain neuro’s and don’t deal with wiring anyway so this eventual appointment will either be really helpful or an utter waste of time and end of the road on any medical help for me. I could cry. But I’m too numb or dead inside or something.
Footnote: Magic Dude is a, er, magic dude! He’s been getting me out of the house whenever he can in any ways he can think of. I have noise reduction ear-plugs which reduce volume and help my processing and migraine management. So he’s taken me to the cinema, a concert, the Outdoors. We’re sick of sitting in coffee shops but that’s all I can do most of the time. But coffee shops exist within garden centres so that adds some extra interest (and buying plants is a temporary retail high). I’ve posted pics for my friends of anything I’ve seen outside the house to share that moment of joy but realise that doing so hides what’s really going on. But there’s nothing they can do anyway, and I’m struggling to read and understand stuff as well as piecing words together to form a reply, so messages can actually be quite stressful if they require a reply.
Oh. I’ve just re-read that list and realised that it’s basically what was happening when my Mum was trying to suss stuff out, got totally wrong concepts about me and disowned me despite my repeatedly saying that I didn’t understand what was going on. Okay. Arse! I’m back there then, eh? Big neuro downslide. Right. I came back a fair amount from that one, let’s see if I can pull the rabbit out of the proverbial hat this time as well with more help than just flukey luck back then when I found I improved a tiny bit from (unknowingly phenylalanine-ish) cheese sandwiches!
Depression is kinda like drowning – it doesn’t look like what you think it looks like. It’s smiling whenever I can, making lots of jokes, going full-on distraction when I’m alone (Lord of the Rings Online), pretending I’m okay just to try and get through until the appointment that’s many months away, yet to be scheduled and which might utterly let me down.
But it might not. ‘Just keep swimming’, right? Ugh!
Next morning: I just re-read this to make sure it made sense then opened something else up on my computer. I felt like had been doing something else but couldn’t remember what and it was really bugging me. I had been re-reading this. Like, a second before and couldn’t remember doing it. And yet after writing this post yesterday my brain accessed the disowning distress from years ago, pulled Bjork’s ‘State of Emergency’ out of it’s vaults and sang it to my dysfunctional fight or flight self til 3am. Gawd this supplement had better help!
.
Okay, the DL phenylalanine arrived yesterday: 25th May 2018. Let the experiment begin. I’ll come back and add how this list looks in a couple of weeks….
Day 1: Shortly after taking the supplement I found myself skim reading two articles in the Psychologist mag, whuuut? Then my brain keeled over, back to ‘normal’.
Day 2: Already using my brain trying to post this when I took the tablet. That weird head tensiony not-headache going on. Not sure I’ll get much impact this morning.
…..
20th June 2018
Okay. Phase 2 started about 5 days ago. Here’s where I’m at:
No major changes on just one tablet per day so phase 2 is an increase to two (one after breakfast and one after lunch, though with health varying these meals vary pretty wildy timewise).
However, I didn’t mention something in my list of symptoms above because if I listed all my symptoms you’d fall asleep trying to read them! Yet it seems to have improved a bit since taking the phenylalanine. No idea yet whether this is causal or coincidental, time will tell.
The unmentioned issue is that since my fall injury I’ve been reacting badly to certain things. I experience near-syncope, nausea, facial drooping, limbs powering down, slurring, eyes flickering independently of each other, dystonia in my legs. The triggers all seem to be when there’s too much for me to process i.e.:
motion (in a car, worse on narrow and/or windy roads, first person gaming)
flickering lights (florescent, daylight through trees when I’m travelling)
audio input at the same time as motion impacts harder and quicker (e.g. music, radio, audio book)
I’m hoping the supplement is related to the improvement in how well I cope with motion. All I can do is keep working through phase 2 and see what happens.
…
Update: 16th September 2022
The phenylalinine really helped….until it didn’t. And I didn’t know why. I now do…
Guess who has chronic brain inflammation?!
Ohhhhh, that explains a lot, eh?!
Systemic inflammation is a Thing with CRPS although I experience very little visible inflammation. In my case inflammation was apparent during the 1st year of acute CRPS but during the subsequent 22 years of chronic CRPS it’s not been visibly apparent unless I experience a trigger like an insect bite and then holy moly! I figured it can’t be that bad in my body. Erm, yeah.
So anyway, imagine inflammation that is untreated and unchecked. I’ve been going to my various GPs over the years asking for help with my concerning neurological issues for well over a decade now. They have never been interested. To find out only once I’ve given up on expecting healthcare for complex multi-systemic patients to suddenly be a thing is kinda gutting – if only they’d listened, right? If only they’d considered the implications of the symptoms I was experiencing, and which were continually getting worse…for yeeaaars. If only. But instead I only found out when I paid someone to assess me who is trained in coming at complex health conditions from a complex and broader viewpoint.
I’ve written about how this discovery came about here.
I received a hand-made Christmas card from a friend I haven’t seen for ages. It gave me such a lift.
Enter a caption
Now I find myself hopefully checking the doormat every day during the run up to Christmas.
Being chronically ill means we’re often lonely. We’re feeling separate from the world that we used to move around in. Every day I check the doormat because a card sitting there would be such a wonderful lift and would help me cope with the long symptomatic Groundhog Day stretching ahead of me. The thing is, it’s hard to write cards when you’re chronically ill. Using what little functionality you have to do so means you can’t do other things. Which is the same for everyone of course but when it comes to illness it’s not about losing time it’s about losing functionality to do something really key, like being able to eat dinner. And whereas missing out on basics like eating isn’t the best for healthy folk, it’s much more severely impacting on an already malfunctioning body.
From a healthy person’s perspective, it’s not that they’ve consciously decided not to send us a card any more for Christmas, birthday or whatever the occasion may be. Well, okay, for some people it might be. It’s not an unusual human response to think that they’re not going to send cards to people who don’t send cards to them, but mainly it’s very usual to not understand what it’s like to be chronically ill.
Being absent from friend’s lives makes us fade into the background because they have other friends they see regularly. Whereas for us, well, we don’t generally get to see our friends. Travel is erm, difficult (one heck of an understatement, I know) so we see whoever we actually live with… and medical practitioners. (Sooo many medical practitioners). Oh and walls. And ceilings (those of us with Dysautonomia tend to know some of our ceilings in quite a bit of detail)! We don’t tend to get to see anyone else. So the friends we haven’t seen for years can be just as important to us now as they were back when we were able to see them in 3D. They do not fade into the background because our foreground is mostly illness, they stand out in the bright and colourful areas that we like the most.
Potentially a healthy friend and a chronically ill friend can perhaps feel very differently about each other. And it’s hard to feel ourselves being faded from their main friend space when they are often still our main friends.
We can’t help hoping for indications through the post that maybe they haven’t forgotten us either, that even though we are ever-absent from their lives that they still somehow care meaningfully about us.
There is a paradox when we make that massive effort though… “I’m determined to write cards this year…” knowing full well that we’re going to make ourselves more ill by doing so: the cards that plop onto the doormat are more often a response to the card we sent rather than something that would have been posted otherwise. So then all that effort brings us a bitter-sweet moment. A card that is meaningful to us and yet never would have arrived if we hadn’t managed to send one ourselves. We learn that when we can’t write cards there are very few people who will still remember us regardless, but we push ourselves every year because we want to send people some love. We don’t write cards to receive them, that is most certainly not the point. We try to write them because our friends mean so much to us. It’s human to feel somewhat bereft when it appears that regard between friends has become imbalanced and yes it’s not actually about cards at all, despite how we tie ourselves in knots trying to work out if we can physically afford the impact from writing them. It’s about connecting with friendships at meaningful times. About feeling loved and included. That we’re still of some importance or significance to them. And it’s about feeling a little less alone at a time of year when loneliness can be most difficult.
In the end we have to be kind to ourselves. If it’s going to reduce our functionality to the point of being even more impaired in meeting our most basic needs then we shouldn’t be pushing ourselves to do it. The reality of not receiving any festive cards is an extra sadness in the overall cruddiness that is being really ill all the time, but we really need to manage our health. Fortunately our pals who also happen to be fellow patients totally get it, we support each other and reiterate our friendships online. Thank goodness for the internet! Though we still try, and each year some of us will succeed in writing a few cards and asking someone else to get us stamps and post them for us.
Interestingly, I find that my doormat is more likely to be graced by completely random arrivals that have nothing to do with yearly events. These are perhaps the most beautiful and lifting kind. When someone has thought of you just because they have, not because you’re on a list. The arrivals tend to be from a few astoundingly thoughtful friends who I either rarely see or have never even met in 3D. These are the heartwarmers. The ones who make us smile just by thinking of them. They are most commonly fellow patients who understand in depth what living with chronic illness is like but who send something because of the love in friendship, not because of the illness we might share (even when what they send may in fact be totally related to our illness, and is super thoughtful and aware because of that too). These arrivals are overwhelming because we know how much it has cost them to do this, and they chose to do it anyway. Love is priceless.
Like these metal drinking straws sent to my by ‘The Princess in the Tower’ so that I can still get some enjoyment from a cup of tea when I cannot raise my trying-to-faint head.
The other arrivals are from that rare breed of healthy friend who sees the health stuff, does their best to understand it but still sees us in here as well. We’re not just a walking illness to them, we’re a friend they love. And because they love their friends, seeing us so ill pains them terribly. But seeing us in here too, gives them hope and helps them cope with the illness stuff. They have to keep their distance to cope, but they don’t stop caring. I don’t think they know just how rare they are, many patients can count these friends on less than one hand.
Contact from those who still genuinely know us and who handle the illness that comes with us as best they can (effortlessly, in the case of fellow patients) means more than a token reciprocal card. People are insanely busy at Christmas. We get forgotten because they are buried in Stuff and they don’t actually see us in 3D. But those blanket text messages and occasional private social media messages that we receive instead mean the world to us. After all, we do the same. It’s better for our health to do it that way and we know that our sentiments are no less for having sent them out en masse, so we know that receiving friends’ messages like that are just as genuine. We may not be able to hang them up and look at them from wherever we are stuck dealing with symptoms that day, but they warm our hearts nonetheless and that’s way more important than warming our doormats.
The yearly paradox persists though simply because it’s nice to be able to send cards to the people we care about. To show we are thinking of them and give them something they can put up in their home instead of read once on their phone. We’d like to be able to be a bit more present in their lives that way. And we’d like to experience being on the receiving end of that, too. Let’s try to be kind to ourselves and allow us to send the messages to those we love in lieu of writing symptom-amplifying cards, or sending a selection of carefully chosen emojis or a voice message in the case of those patients who experience enormous impact from using their hands. Says the hypocrite sat here surrounded by cards that I hope to write.
Yep.
Every year. <headdesk>
Happy festivities to you all whichever they may be. Be kind to yourself, there are people out here wishing you well and who are dancing the paradox with you.
I damaged my coccyx back in January but I have a pre-existing intractable pain condition (CRPS) so I don’t show how much pain I’m in. It’s a habit that’s developed over the past 18 years of living with severe pain all of the time. Only my boyfriend can clock when the pain is beginning to soar, those of my friends who think they can see when I’m in pain have no idea that by the time they spot it I’m on the verge of inward screaming.
So if my own friends cannot see how much pain I’m in how is a doctor who rarely sees me supposed to comprehend my reported pain levels when they don’t match my outward appearance?
Most practitioners (including pain management teams) will use the 10 point pain scale. But it’s hard to convey what our understanding of that scale is.
When I was first seen by a pain management team aaaall those years ago I was told that a 10 was the worst pain that I could “imagine”. I’m pretty imaginative! And besides I figured that even though I had reached the stage of realising that if someone offered to chainsaw my legs off with no anaesthetic that I would have said ‘yes’ in my desperation I still figured that there must be experiences out there that are even worse than that. So I rated my pain at a 6 when I now know it was a baseline 9 with regular 10s.
When I had completed the maximum allowed NHS pain management treatment time I knew that my baseline pain had reduced a bit so I felt I ‘had’ to rate it less than my starting ‘6’ so I rated it at a 4 when it turns out I was actually getting discharged at a dreadful baseline (i.e. what our pain levels never drop below) of 8. So yeah, the team probably thought they did pretty well and I didn’t know why or how they expected me to be pleased and able to cope/function thereon after. *sigh*
Miscommunication is easy when a scale is subjective.
Being told that a 10 is the worst pain we’ve ever felt doesn’t usually help much either as with a severe 24/7 pain condition the likelihood is that thisis the worst pain we’ve ever felt and that just leaves them with a 10 which they often don’t feel is very helpful even though we’ve answered within the parameters.
So… I figured (years later) that I had better find some descriptors for each number on the scale. That way I could share those with my doctor so they could see what pain levels each number represents for me. It makes it easier for them to understand what their patient is actually dealing with so it’s useful input for their assessment.
I collected various descriptors from multiple medical sources and started recording my pain (and other symptoms) in accordance with these. My doctor ended up with several weeks worth represented in one easy-to-assess graph which showed clearly my pain baseline as well as how often and how high the pain spiked (I wrote about that, and first shared my less prettified pain scale descriptors, here). Doctors have a mere few minutes to talk with us so it is helpful to be able to present data in the most accessible way for us to get the most out of an appointment and for them to best be able to understand and help their patient in the time allowed.
It helped me. It helped my doctor.
Especially as my high level intractable pain has been with me so long that I tend not to ‘look’ as bad as I feel. Though after making it to the surgery, through a conversation and then home again I usually find that by heck it shows by then. The doctor doesn’t get to see that bit because we chronically ill have to be at the best we possibly can be to be able to hold a conversation well enough for the meeting to be useful. It is necessary and yet very misleading.
So, here’s my compiled pain scale descriptors in a more user friendly format that when I first wrote about them. I hope that it may prove useful to patients and doctors alike. The reason the compilation is more helpful to me is because when one aspect of it doesn’t pinpoint it well enough another aspect will help me figure out where I am on the scale. Pain interferes with decisions, assessments, pretty much any processing to be honest! So I find that the higher pain level I’m at the less capable I am of accurately placing it on the pain scale. Particularly helpful to me when I’m really bad are the points at which tasks and then concentration get affected – I know that tasks are being affected but when my concentration is being affected it takes longer for me to actually realise that the reason I’m struggling to pinpoint my pain is because… my concentration is being affected!
A fellow expert patient and ex-nurse pain blogger, Isy Aweigh, also wrote about the alternative option of personalised pain scales here, which is well worth a look.